

I am not one to do “lists” often, but I feel it is warranted given the new force to bring back masking. Our leaders tried to do this last year with covid ramping up and it failed. I do think they won’t get the compliance again, but it is interesting to see the covidians still cosplaying pandemic theatre in 2023. I have done posts in the past describing ad nauseam how masks are ineffective for stopping the spread of viruses, including covid, in 2020, 2021, and 2022. This was all but confirmed with the Cochrane Study on masks, produced in 2023, outlining:
“The pooled results of RCTs did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks. There were no clear differences between the use of medical/surgical masks compared with N95/P2 respirators in healthcare workers when used in routine care to reduce respiratory viral infection.”
Now, in many of my blogs I have pointed out the best studies to determine if masks were effective, some studies had many issues, but they told the conclusion: “through higher-order studies, masks are not a statistically significant measure to stop the transmission of COVID-19 or any other respiratory virus.” But to poke fun at covidians, and their fealty to mask-wearing, I think it is time to look at the worst studies that were produced on masking, some of these studies more recent, and still keeping covidians at all stages wanting to bring back masks, and yes, some of leaders in hospitals and school boards are bringing back masks in 2023.
The Studies
10. Chan et al. (2020). Surgical Mask Partition Reduces the Risk of Noncontact Transmission in a Golden Syrian Hamster Model for Coronavirus Disease 2019 (COVID-19). A.K.A. the hamster study. [Study]
What can be said about this study? Well, the most glaring is that they somehow simulated mask-wearing on hamsters and figured this was akin to human characteristics of mask-wearing, but what are some key areas within the study that make it so bad? Well, retracting my previous statement, they did not get the hamsters to wear masks, they determined masks work by putting covid infected hamsters in one chamber, non-infected ones in another, and “a polyvinyl chloride air porous partition with unidirectional airflow within the isolator” as the mask effect.
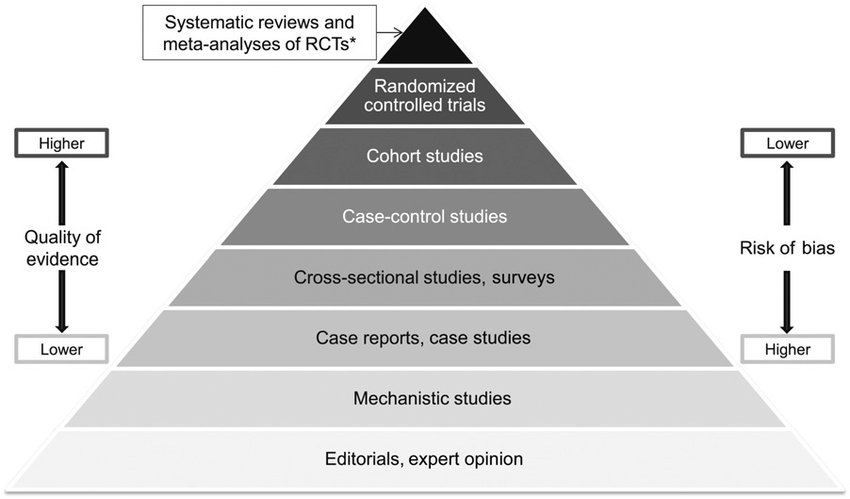
What makes this study bad, is that it is used to justify that masks work, even though transmission only had a marginal effect. But the worst is that it is largely a mechanistic study which falls lower pyramid of evidence meaning a lower quality of evidence and a higher risk of bias. Consider this pyramid of evidence for future studies we discuss, as it is an important factor for assessment.
9. Cowger et al. (2022). Lifting Universal Masking in Schools — Covid-19 Incidence among Students and Staff. A.K.A. the Massachusetts school district study. [Study]
The methodology for this study was a policy differential analysis between school districts in Massachusetts in 2022. They wanted to assess and compare school districts who implemented mask mandates, against schools that did not implement mask mandates. The study concluded that districts that lifted the mask mandate, were “associated with an additional 44.9 Covid-19 cases per 1000 students”. At the outset you may think this is significant evidence of mask effectiveness given that differential analysis is seen as some gold standard amongst covidians akin to a randomized control trial, but as you will see it is with its significant biases.
Tracy Beth-Hoeg (@TracyBethHoeg) – an epidemiologist at the University of California San Fransisco – does a good job at dismantling this study on many fronts. She concludes that prior immunity played a big factor in the masked individuals, meaning the stringent masking did not reduce transmission in the least. What Beth-Hoeg et al. also found was that the Cowger et al. study cherry-picked certain districts to confirm biases, when Beth-Hoeg et al. analyzed all 306 school districts in Massachusetts – instead of the 70 in the Cowger et al. study – they found that infection rates were not statistically significant, and in actuality, districts that got rid of the mask mandates had larger decreases in infection due to infection-induced immunity, see the many studies on T-Cells.
The Cowger et al. study was used a lot on mainstream media sources as a justification for mask mandates working. I think the failure of these individuals to understand how studies work and what they actually say was a problem with this whole narrative around covid. So much so, to brush off clear biases in the research and distort the actual findings.
8. Ginther & Zambrana. (2021). Association of Mask Mandates and COVID-19 Case Rates, Hospitalizations, and Deaths in Kansas. A.K.A. that early Kansas study touted by the CDC. [Study]
This study used a case-control methodology, which is on the higher end of the pyramid of evidence, with medium quality and medium bias. They used data from the New York Times and the Kansas Department of Health and Environment for their data. Essentially their case-control did not use any impactful processes, just merely wrote comparisons adjusted for population. Using linear regression models they found that counties that implemented mask mandates had an equivalent of a 60% reduction covid cases for masked counties compared to unmasked counties.
Now, most people who read this may be intimidated by the usage of words such as “linear-regression model”, or “case-control methodology” as it presents interesting numbers and algorithms that are confusing to the layperson. However, a famed quote by Leonard H. Courtney – popularized by Mark Twain – gives a precursor to the discussion of this study “lies, damned lies, and statistics.”
That bad cat El Gato Malo (@boriquagato) – is an anonymous feline on Twitter, but shows the hallmarks of a Ph.D. in Mathematics – dismantles this study. What he points out is that the linear regression model is only as good as the variable put in, when those variables are cherry-picked it can present a flowery image that is not quite true.
What you can see from the graph is that the linear regression placing a certain time frame with invalidated controls, rendered results positive for mask use, but when extrapolated you will see, once again, there is no statistically significant difference between masked and non-masked counties for case incidence. This study teaches us to be careful with linear regression statistics, as they are only as good as the biased data put in by researchers.
7. Brooks et al. (2021). Maximizing Fit for Cloth and Medical Procedure Masks to Improve Performance and Reduce SARS-CoV-2 Transmission and Exposure. A.K.A. CDC Double-Masking Mannequin study [Study]
This study was listed as a Morbid and Mortality Weekly Report (MMWR) highlighted by the Center for Disease Control and Prevention (CDC). The MMWR attempts to provide rapid trials or reviews to be released immediately on the CDC website as guidance for health. During covid, the MMWR was impactful in guiding individuals and organizations (both government and private) on how to handle the pandemic, and if need be, implement mandates. However, the obvious issue with MMWRs is that they are rapid releases, meaning the methodology and controls are rushed, leaving no room for deep analysis. Much like this study, using mannequins to simulate particle distribution when ‘simulating a cough’.
Vinay Prasad – hematologist and oncologist at the University of California San Fransisco – goes through this research with a fine tooth comb outlining the pitfalls of the research, such as how uncomfortable the masks are when a human is talking, not a mannequin with a hose attached to its mouth. Journalist Jordan Schachtel outlines that even the study noted the limitations on how this would affect humans, such as “double masking might impede breathing or obstruct peripheral vision for some wearers.”
The biggest limitation, or flat-out absurdity of this study, is that it shows that double masking would stop large droplets from a cough or a sneeze – well of course, so does a Kleenex. However, this was after it was confirmed that covid is a fine aerosolized virus that can linger for hours and is microscopic compared to the threading of masks. For example, here is a video showing how our breath, which carries and transmits virus particles – can easily blow out a candle even with double-masking.
6. Leung et al. (2020). Respiratory Virus Shedding in Exhaled Breath and Efficacy of Face Masks. [Study]
I have a personal vendetta with this one as it is not commonly talked about but has all the hallmarks of a bad study. They used a simple screening process – somewhere in the middle of a case report and a mechanistic study, higher risk of bias and lower quality of evidence – and found that out of 246 individuals half provided breath samples with a mask and without a mask. What the authors found were significant reductions in respiratory droplets from mask wearers compared to non-mask wearers. With some fancy graphs, covidians in early 2020 were able to convince people that wearing masks, any mask, can limit the spread of coronavirus.
Unfortunately, this study was bad then and it is even worse now. First, we know covid is spread through tiny, aerosolized droplets rendering the controls for this study moot, as they swabbed for large viral droplets. Second, and most concerning in my book is the obvious p-hacking that the authors did to get the significant results they wanted. For those not familiar, p-hacking (data dredging) is a form of academic dishonesty where researchers misuse data to find patterns that are statistically significant through numerous statistical tests, hacking (or dredging up) the statistically significant ones and ignoring the others.
The authors took numerous samples from the participants but only used one average sample in their charts and tables. You can find statistically significant findings in anything if you do numerous tests, and find one average sample for all of them. For example, I can say that traffic is busy on Main Street on Tuesdays. Now most Tuesdays it is not busy, but if I take multiple samples, I am bound to find a busy day, and when I average them, the mean (μ) ends up being skewed.
- Tuesday 1: 3 cars
- Tuesday 2: 3 cars
- Tuesday 3: 10 cars
- Tuesday 4: 45 cars (construction on Outer Street rerouted cars that day)
- Tuesday 5: 3 cars
- Tuesday 6: 3 cars
- Tuesday 7: 6 cars
- Tuesday 8: 4 cars
- Tuesday 9: 4 cars
- Mean (μ): 9 cars
What we can see in this example is that my mean would suggest that Tuesday is busy on Main Street averaging 9 cars. Say in my statistical study 9 represents a significant finding for busy traffic, whereas 4 or 3 would be regarded as insignificant. Well, the mode would be a better representation of the data here suggesting that 3 is more representative of the traffic than 9. One participant in the Leung study could have had more symptoms of coughing and sneezing thus causing an outlier that rendered statistically significant findings.
I think why this one is upsetting to me is the blatant dishonesty in the findings and that this study has not been retracted. I think a consolation prize is that it has been rendered useless given the knowledge of how the covid virus actually transmits.
5. Aabaluck et al. (2022). Impact of Community Masking on COVID-19: A Cluster-Randomized Trial in Bangladesh. A.K.A. Bangladesh Mask Study [Study]
Full disclosure, I used this study in my significant research blog since it is an RCT and considered significant research. With that said there are still some significant problems with the study, and should not be considered on the level of the Danish Mask Study for example. Even with RCT methods and a bias from the author, they still found masks were largely ineffective and not statistically significant in reducing spread. Such as the conclusion that only 60+ saw a reduction in covid, but not other age demographics.
Some interesting outcomes that came from the study showed that only a 9% reduction came from mask-wearing wearing which is not statistically significant, and the authors did not obtain good seroprevalence data to confirm infection. Again, based on how one will interpret the data, if two areas, one masked, one unmasked, measuring covid and only having a difference of 20 cases per 2000 is not enough to say that masks work, considering extenuating variables. For example, that is like saying the unmasked had 2000 covid cases, whereas the masked control only had 1980 covid cases – therefore, masks work? That is an incorrect statistical analysis.
4. Lam-Hine et al. (2021). Outbreak Associated with SARS-CoV-2 B.1.617.2 (Delta) Variant in an Elementary School — Marin County, California, May–June 2021. A.K.A. Marin County Teacher Study. [Study]
Another MMWR report with a methodology that is unclear in its scope, but after reading the study we can just chalk it up to an observational case report (low quality, high bias). It found that a teacher inside of a Marin County school who removed their mask while infected spread the virus to 12 out of 24 students. Of course, no data is supporting how it was the teacher that spread the virus, or how was it that when the students entered the classroom, it was only when she removed the mask the kids got infected. The MMWR justifies it because they come from a bias that masks automatically work so it must have been when she removed the mask.
The confirmation bias in this MMWR is staggering, and considering it was CDC-approved, it belongs on a conspiracy website for covidians. Not to mention at the time of the study a large proportion of Marin County residents, including children, were vaccinated against covid, and the county still had one of the strictest mask mandates in all of the country. Logic would deduce highly vaccinated, mask mandate, and the county still had an outbreak of the delta variant – enough said.
3. Boulous et al. (2023). Effectiveness of Face Masks for Reducing Transmission of SARS-Cov-2: A Rapid Systematic Review. A.K.A. Royal Society Mask Study. [Study]
This is the most recent/absurd study on masks for covid published in the 2023 Royal Society report: COVID-19: Examining the Effectiveness of Non-Pharmaceutical Interventions. Not only did the report give positive praise to school/societal lockdowns (regarded as universally harmful here, here, here, and here), but they also supported the NPI of mask-wearing as generally stopping covid spread. They did not use good studies like Cochrane, or the Danish Mask Study, they used the Boulous et al. study – so naturally, the study needs to be reviewed.
Of course, this study strongly suggests it is a “rapid systematic review” of the evidence regarding mask-wearing. However, it is in the selection of studies that it falls apart. Out of the 35 studies selected, 32 were observational studies (akin to case reports: high risk of bias, low quality of evidence), even the study itself admitting that the observational reports held 91% critical risk of bias, something that was explained, but subverted in the Royal Society report. That is the common misconception with literature reviews, not all are considered good in the sense, that the literature review is only as good as the studies that are added – and with a cacophony of bad studies can render a bad literature review.
Ultimately, the Royal Society study reinforces that global leadership has not learned their lessons from their pandemic errors, or they know the errors, just unwilling to admit they were wrong, and would rather double down on their errors. This is not a logical fallacy anymore, this is pure and blatant narcissism.
2. Hendrix et al. (2020). Absence of Apparent Transmission of SARS-CoV-2 from Two Stylists After Exposure at a Hair Salon with a Universal Face Covering Policy — Springfield, Missouri, May 2020. A.K.A. Missouri Hairdresser Study. [Study]
The reason why this MMWR is rated so high is that it was the original study on masks that the CDC used in early 2020 to recommend mask mandates that lasted in some places for over 2 years. Not only that but it is considered one of the worst studies conducted in terms of methodology and outcomes. It is true to say that millions and millions were masked because of junk science, and it all stems from this paper.
The methodology is quite simple, confirmation bias with a dash of poor control parameters makes this study one of the most flawed out there. Out of the 139 clients observed who came in contact with the masked hairdressers, only 48% were tested for covid, and all came back negative. The authors conclude that this must mean that masks work; however, it is not that clear as you cannot confirm something has worked when only 48% of the respondents test knowing the errors with PCR testing. 52% could have contracted covid, and of that 48% could have contracted covid, and when they tested they were cleared of the virus. Many variables are missing here, and it is astonishing that the CDC still has this study up.
Eric – unknown position, but says he has a background in biomedical engineering – offers excellent additional criticism to the study, such as the Missouri DHS process of the study came back after cases decreased without mask mandates to show that masks in this window worked, but it was actually due to natural virality patterns.
Overall, the Missouri Hairdresser study was used by covidians as the gold standard for suggesting mask use stops covid, unfortunately in 2023 we know that not to be the case, and is seen as ridiculous now. But the most troubling aspect is that our leadership saw this study and decided to give it the royal decree of truth. I could care less about this study now, the work needs to be done to point out studies like this in the future and make sure they are not inflated by our leaders again.
1. Howard et al. (2020). An Evidence Review of Face Masks Against COVID-19. A.K.A That Jeremy Howard Covidian Study [Study]
Some would rightfully argue that the Missouri hairdresser study should be number 1, and in many cases, I can agree with them. But if we want to know why the covidians were emotionally set on mask-wearing, it is found in the Howard et al. mask study. This study is used by pretend smart covidians as a gold standard for some reason, and it most certainly should not be.
First, this is considered a narrative review which on the hierarchy of studies is quite low for quality and high for bias, and it shows. The authors made a point to find only stories relevant to the studies that meet their ideological framework even though there were many studies before, about 170 to be exact, that show masks are ineffective in stopping respiratory viruses. What is interesting is that even when the covidians want to add observational studies and narrative reports, we are fine with that, because not only are the Randomized Control Trials (RCT) and Systematic Literature Reviews (SLR) on our side, but so are the majority of the observational cohort, case studies, case reports, and mechanistic studies are on our side as well.
Granted, this was in early 2020 almost 3 years before the Cochrane study, and the authors admit that RCTs and SLRs are needed for a proper evidentiary finding. Well, that time has come and it renders their study obsolete. The authors even mention studies that show masks don’t work, but it was not related to covid so it doesn’t count – even though covid has the same viral makeup and dynamics as other seasonal coronaviruses. So yes, the 170, and now more, studies related to masks not working for respiratory viruses count for covid, to omit them based on a different name is irresponsible.
What is telling about this study’s errors is that they recommend household face masks to protect against respiratory viruses (i.e. a shirt, a bandanna, a piece of cloth, etc.), the effectiveness of homemade cloth masks has been proven ineffective time and time again, even the CDC admits this.
This study also heavily emphasizes modeling, which I point out in my early analysis on covid as an ineffective way to judge human behavior and use in policy creation. But it is the final part of the study that calls for a collective symbolism around wearing a mask, insofar that it shows that you are ‘doing the right thing’. This is a political statement, not scientific evidence, this is not even a good sociological methodology. In the future, I will consider discussing the political impact covid had, which I feel was the whole consideration for the pandemic in early 2020. But, for now, we can look at the outcomes of this study as wildly exaggerated, extremely biased, and based on political motivations rather than scientific inquiry – hence, in my book, the worst mask study ever produced.
Implications and conclusions
What can we draw from these studies? Even if a covidian reads this, at this point, they will cede to the narrative, they will downplay and deflect just like they have always done. Which makes one wonder, why even write something like this. I am a proponent of history repeating itself, meaning it is always good to have something in case the lunacy comes back. It seems around every August-September a news article comes out wondering if we should mask up again. This means that our leadership has not learned their lesson and needs to be constantly reminded of their error, until they acknowledge they were wrong in all areas of pandemic management: masks, lockdowns, vaccine mandates, suppression of opinions, etc.).
Another problem is the lack of ethics in research, processes like biases with linear regression models or p-hacking would be grounds for retraction, in more serious instances, a total discrediting of a researcher that would follow them for quite a long time. According to the Washington Post, Morning Consult, and Pew Research, Americans’ trust in public health has steadily declined and continues to decline in the wake of the pandemic. This has many factors, the flip-flopping of guidance showing a lack of critical knowledge, leadership embracing a ‘rules for thee not for me’ mentality while they enjoy the fruits of life while we were locked in our homes, the massive corporatization of medicine where companies like Pfizer and Moderna act more like sleazy car salesman than pharmaceutical organizations.
Now I know this post was only about masks, but this is a microcosm of a larger issue involving public health. If the public health establishment wants to start mending the relationship with the citizenry, admit the faulty analysis on masks and admit to your mistakes.

{kind=link}
Hello from the UK
Well said. I have been trying to persuade the mask-ists (!) that masks are pointless. Some people seem to welcome them back at the moment which I find unbelievable. I did my own humorous take on masks back in 2020 updated in 2023 should you be interested.
LikeLike