
A recent post from the Twitter handle NYC Angry Mom – please follow her @angrybklynmom – posted quite a salient thread that everyone needs to read. It has been something I have been waiting to see; a compendium of all the social media backlash from concerned COVID doomsdayers who cannot comprehend good news and are gripped by fear. Full disclosure, I feel bad for these people and I wish they would make plans to get help for their anxiety, but alas, with the variants being the most recent, ongoing, and probably last topic of discussion for the COVID saga, I find this will be my opus in my over year long blog topics on COVID. After a year of scolding, quietness, and ultimately justification, I have grown tired of the continual banter that comes from social media doomers and this is a final list of concerns continually brought up with effective answers.
“Masks prevent the spread of droplets.”
Yes, masks do have the ability to stop large droplets from a cough or sneeze which is basic viral dynamics, much like if you took a pebble and dropped in on the inside of a mask the mask would stop that pebble from going through. However, COVID is spread through microscopic aerosols much smaller than the threading of a mask. Dr. Byram Bridle confirms this in a video posted a few months ago discussing the effectiveness of a mask through a real-world simulation. This is all but confirmed through studies done in Denmark and a pre-print recently released from the United States. Also, Oxford University’s Center for Evidence Based Medicine compiling a release of pre-2020 studies that confirm the Danish and American studies.
“Get vaccinated, natural infection does not offer good enough immunity.”
This is false, natural infection along with vaccinations render the same amount of immunity against the virus. This is confirmed through a study done by the Cleveland Clinic and the numerous studies done on T and B Cell immunity dating back to last summer.
- https://www.nature.com/articles/s41586-020-2550-z_reference.pdf
- https://www.nature.com/articles/s41586-020-2598-9_reference.pdf
- https://www.nih.gov/news-events/nih-research-matters/immune-cells-common-cold-may-recognize-sars-cov-2?fbclid=IwAR20MQaEu_m64mWJkHxSVkCqxsF_vRtifrD_lWQBErM9UxC_yySzo9q-4tQ
- https://jamanetwork.com/journals/jama/fullarticle/2770758
- https://www.bmj.com/content/370/bmj.m3563
- https://www.cebm.net/covid-19/what-is-the-role-of-t-cells-in-covid-19-infection-why-immunity-is-about-more-than-antibodies/
- JAMA Article
- https://doi.org/10.1016/j.ebiom.2021.103410
“Natural infection does not work against any variants and variants are more transmissible and deadly.”
Research determines that this is untrue as reports out of JAMA and Oxford have confirmed that the vaccines and natural infection are quite effective with wild-type, current, and future variants given that future variants are genetic mutations from previous variants. This is on top of the study by Lucy Van Dorp who suggests variants don’t carry the transmissibility as frequently described. It is also important to look back at the Cleveland Clinic study which was conducted during the height of the UK variant. Also, most recently, a report was released by the UK government with hard data relating to the delta Indian variant. What was found is that a Case Fatality Rate (always higher than Infection Fatality Rate) rendered a range of 0.2-0.4% or 32 deaths, much lower than the UK variant during the winter which rendered 4295 deaths.
“Even still, patients can suffer from Long-COVID”
The concept of long-COVID is debated and aside from scant anecdotal evidence, long-COVID is generally non-existent. Two reports from the BMJ in mid-2020 reflect that some long-term symptoms may exist; however, like other viruses, they are rare and statistically insignificant with sparse findings of fatigue lasting three weeks after infection and older, co-morbid patients showing the most symptoms at times beyond a month – less than a month and a half. This was before new evidence emerged on the psychological impact of long-COVID and how it may be more of an influence through a marshalling of epidemic authority, and a sense of togetherness during an anxious time rather than viral symptoms.
“Look at the cases, they are going up!”
The difference is that cases may go up, and they may continue to go up. However, since I have been observing COVID it is important to distinguish between five characteristics of status:
- Case: A positive PCR test run between 35-40 cycles.
- Hospitalization: A confirmed case of COVID via a hospital visit for COVID or for another issue.
- Hospitalization and ICU: A confirmed case admitted to the ICU expressly for COVID.
- ICU and Ventilator: In ICU and intubated with low oxygen levels.
- Death: A death certificate confirming death by or with COVID. (CDC 3 co-morbidities)
Through an apparent ‘old standard’ of pandemic case control, Jay Bhattacharya once suggested a rule of 3 to confirm a case of a viral pathogen: symptomatic, done at a hospital, positive test. It would seem that more cases were found given the massive rollout of PCR testing which was outlined in the New York Times and confirmed in a study out of the UK. This ultimately causes an inflation in cases, much like the UK now with testing happening to all school aged children.
“It’s just masks and distancing for a short time.”
In most places 16 months is not a short time, and now with doomers wanting to return the mask mandate, it is important to reiterate the mandates did not work as outlined in this image showing mandates implemented (red dots) with the case trend of 11 industrial and Northern Hemisphere countries for continuity.

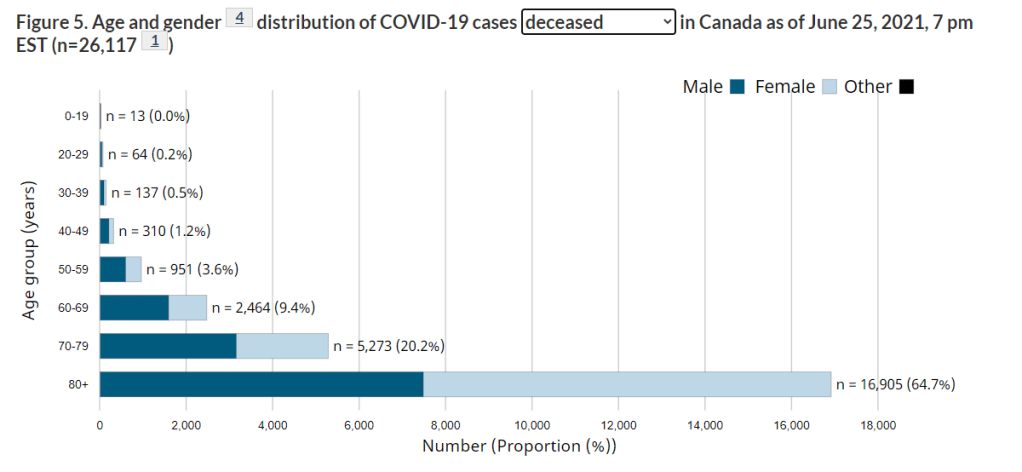
“This virus doesn’t discriminate.”
It very much does, and its discrimination is age. Out of all the death counts around the world a large majority of deaths happened to individuals over 70 and in some countries over 80 was the largest cohort. This is a clear data point to focus strategy on protecting and vaccinating the elderly and infirm, once vaccination is complete for this cohort the panic should be gone. As you can tell in June/July this is still not the case. Here is the compiled data to date on age stratified death in Canada. If you have the chance, check out your country to see if its similar.
“Lockdowns saved more lives than harmed.”
The team at Collateral Global have intensely outlined the dangers of lockdown with a host of news reports, research papers, and other data to confirm the dangers of lockdown outweigh the benefit. This was further confirmed in a peer-reviewed study that shows no clear benefit to locking down.
“COVID is spread through super spreader events like anti-lockdown protests and sporting events.”
This is patently false considering protests have been happening with anti-lockdown and BLM and no significant data reflects that heightened COVID cases are caused by these events. Also, no significant rise in cases that stemmed from the Super Bowl in Florida or opening day in Texas. This has always been political rhetoric as outlined in this piece from the New York Times.
“Vaccines work, no other treatment has been proven.”
Although the vaccines yield a high efficacy – a recent meta-analysis of randomized control trials provide the clearest and most definitive proof that Ivermectin is effective to treating COVID-19 as a prophylaxis and as a treatment measure inside hospitals. This is a safe alternative to stopping the virus and healing patients who are struggling inside hospitals.
Conclusion
I thank @angrybklynmom for providing a muse for me to create this. If you want this to end you have to meet the irrational with effective and simple answers, also linking to actual research articles are the most beneficial. This places the onus on them to provide contrary evidence in a debate to solidify their points and refute yours. After all, that is what science is. Now I hope this is my last COVID blog because it is tiring to say the least. I think I’ll leave with a meme that perfectly encapsulates my level of frustration along with importance I place on COVID at this time.

